
Why Your Tinnitus Might Be Coming From Your Neck: An Acupuncture Perspective

For many people with tinnitus, investigating the source of the problem follows a familiar path. A GP referral to an audiologist, a hearing test, maybe an MRI to rule out anything structural. Earwax gets checked. But there’s cases where each test comes back clear and the ringing continues without explanation.
At that point most people are told there's nothing obviously wrong with the ears and not much more to offer beyond management strategies. That's often where people are desperate for answers. What tends not to get explored is whether the source of the problem is coming from somewhere other than the ear entirely.
When the ear isn't the source
Research recognises cervicogenic somatic tinnitus as a distinct subtype, estimated to affect up to 65% of tinnitus patients in clinical studies. In this presentation, tinnitus arises not from damage or dysfunction within the ear itself, but from altered sensory input from the cervical spine and jaw region.
The mechanism runs through the brainstem. The neck and jaw connect to the auditory system via a relay centre called the trigeminocervical complex, where sensory information from the upper cervical nerves and the trigeminal nerve converge. When muscles in this region are chronically tight or irritated, they send abnormal signals through this pathway that the brain interprets as sound. The result is tinnitus that has no identifiable ear-based cause.
A useful indicator of somatic involvement is whether the tinnitus changes with movement. If rotating the neck, clenching the jaw, or applying pressure to the upper trapezius or suboccipital region alters the loudness or character of the ringing, that points toward a somatic rather than purely auditory origin. Tinnitus patients are 6.7 times more likely to have temporomandibular joint disorders and 2.6 times more likely to have neck issues than people without tinnitus, which suggests the connection between these systems is more than coincidental.
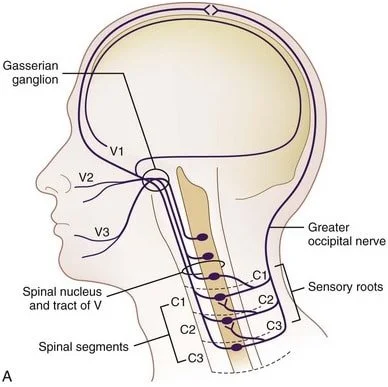
The trigeminocervical complex. Image source: Donald Physiotherapy
Why treating the neck alone isn't always enough
Somatic tinnitus is better understood as a problem of central sensitisation rather than purely a mechanical one. The musculoskeletal findings in the neck and jaw are real and worth treating, but they are feeding into a nervous system that has become sensitised and is amplifying the signal beyond what the original mechanical input would produce.
As one specialist in tinnitus neurology has noted, effective somatic tinnitus care needs to work on both levels simultaneously: addressing the jaw and neck factors while calming the central nervous system reactivity that is driving the amplification. Treating only the neck or only the nervous system tends to produce incomplete or short-lived results.
This is where acupuncture is worth considering. Local needling to the neck, jaw and ear region addresses the musculoskeletal component directly. The systemic effect of acupuncture on the nervous system, including its documented influence on the HPA axis and autonomic regulation, addresses the central reactivity component at the same time. Both mechanisms are engaged within the same session rather than requiring separate interventions.
What Chinese medicine adds to the picture
Alongside the somatic approach, Chinese medicine offers a pattern-based framework for understanding tinnitus that has been documented in classical texts for centuries. These patterns don't replace the somatic assessment but can help explain why some people are more susceptible to persistent tinnitus than others, and can guide treatment when the somatic approach alone is insufficient.
The four patterns most commonly associated with tinnitus in Chinese medicine are:
Kidney deficiency is the pattern most classically linked to tinnitus in TCM literature. The Kidney in Chinese medicine is considered the root of the body's fundamental reserves. When Kidney essence is insufficient, often from ageing, overwork or prolonged depletion, it fails to nourish the ear, which is its associated sensory organ. The tinnitus tends to be low-pitched, gradual in onset, worse with fatigue and at night, and is often accompanied by lower back ache, poor memory and reduced vitality.
Liver Yang rising tends to produce a more sudden onset, high-pitched tinnitus that worsens with stress, anger or frustration. The Liver in Chinese medicine governs the smooth flow of Qi. When chronic stress causes Liver Qi to stagnate and generate Heat over time, that Heat rises and disturbs the sensory organs of the head. Headache, irritability and a feeling of pressure in the head often accompany this pattern.
Phlegm-fire produces a loud, low-pitched tinnitus often associated with dizziness, a feeling of heaviness or fullness in the chest, and digestive symptoms. It tends to develop in people with a history of poor diet, excess alcohol or chronic dampness accumulation. The combination of Phlegm and Heat obstructs the clear orifices of the head, of which the ear is one.
Qi and Blood deficiency produces an intermittent, low-pitched tinnitus that is worse with exertion or after illness. It is associated with general fatigue, a pale complexion, poor appetite and reduced concentration. This pattern is worth considering in patients whose tinnitus began or worsened after a period of sustained depletion, illness or significant blood loss.
In practice, these patterns inform the systemic component of treatment rather than the local approach. Addressing the underlying pattern alongside the somatic work tends to produce more sustained results than either alone.
What treatment involves
The approach here combines local acupuncture around the ear and jaw with motor point work through the neck and shoulders.
Local points around the ear include SI19, TE21 and GB2, which sit directly around the tragus and pre-auricular region. TE17 sits just behind the earlobe at the base of the skull and is used specifically for ear-related conditions including tinnitus and hearing difficulty.
Jaw points include ST6 and ST7, which overlie the masseter and the temporomandibular joint respectively. These are worth including when jaw tension is a contributing factor, which is common in somatic tinnitus presentations.
Neck and shoulder points address the muscles most commonly involved in cervicogenic tinnitus. Motor point acupuncture to the upper trapezius, SCM and suboccipital muscles aims to release the trigger points and restore normal muscle tone in these regions. GB20 at the base of the skull and GB21 on the upper trapezius are standard points for this presentation. TE17 bridges the local ear work and the neck work given its position at the junction of these two regions.
Electro stimulation can be added at the motor points to deepen the release and improve local tissue perfusion where the pattern is well established.
Three things worth considering alongside treatment
Manage stress: Stress and anxiety are known to aggravate tinnitus regardless of the underlying cause. When the nervous system is in a heightened state, the brain's sensitivity to sound signals increases, making tinnitus more noticeable and harder to ignore. Anything that supports nervous system regulation between sessions, regular movement, consistent sleep, time away from screens, is worth building into the routine.
Reduce caffeine and alcohol: Caffeine is a stimulant that increases neural activity and can amplify tinnitus perception. Alcohol initially dilates blood vessels but causes rebound constriction, which can disrupt inner ear fluid balance and worsen symptoms. Neither needs to be eliminated entirely but both are worth being honest about, particularly if tinnitus tends to be worse the morning after drinking.
Get your jaw assessed: Jaw tension and TMJ disorders are a recognised contributor to somatic tinnitus. If the tinnitus is accompanied by jaw clicking, facial tension, teeth grinding or morning jaw soreness, it may be worth having the jaw assessed alongside the tinnitus treatment. These two complaints are more connected than most people realise.
References
Bousema, E. J., Koops, E. A., van Dijk, P., & Dijkstra, P. U. (2018). Association between subjective tinnitus and cervical spine or temporomandibular disorders: A systematic review. Trends in Hearing, 22, 1–16. https://doi.org/10.1177/2331216518800640
Chae, Y., Lee, H., Kim, H., & Kim, H. (2009). Acupuncture point selection based on anatomical considerations for the treatment of somatosensory tinnitus. Medical Hypotheses, 73(5), 692–695. https://doi.org/10.1016/j.mehy.2009.04.044
Djalilian, H. R. (2026). Somatic tinnitus: Causes, symptoms, and treatment. NeuroMed Tinnitus Care. https://neuromedcare.com/somatic-tinnitus/
Langguth, B., Kreuzer, P. M., Kleinjung, T., & De Ridder, D. (2013). Tinnitus: Causes and clinical management. The Lancet Neurology, 12(9), 920–930. https://doi.org/10.1016/S1474-4422(13)70160-1
Michiels, S., & De Hertogh, W. (2023). Somatosensory tinnitus: Recent developments in diagnosis and treatment. Journal of the Association for Research in Otolaryngology, 24(5), 465–472. https://pubmed.ncbi.nlm.nih.gov/37668853/
Ralli, M., Greco, A., Turchetta, R., Altissimi, G., de Vincentiis, M., & Cianfrone, G. (2017). Somatosensory tinnitus: Current evidence and future perspectives. Journal of International Medical Research, 45(3), 933–947. https://pmc.ncbi.nlm.nih.gov/articles/PMC5536427/
What to expect when you visit
The first consultation would start with a conversation about when the tinnitus began, what investigations have already been done, whether the sound changes with neck or jaw movement, and what other symptoms are present alongside it.
From there, the assessment covers the neck and shoulder muscle tone, jaw function and range of movement, and the Chinese medicine tongue and pulse picture to identify any underlying pattern contributing to the presentation.
Treatment is tailored to what the assessment reveals. The combination of local ear and jaw points, neck and shoulder motor point work, and pattern-based systemic points varies depending on what is most prominent in each session.
Tinnitus can be one of the more challenging conditions to treat and results are variable. If investigations have come back clear and the standard approaches haven't produced a change, it may be worth coming in to assess whether the neck and jaw are contributing to the picture.

About Brandon Lau
Brandon is a registered Acupuncturist and Chinese Herbal Medicine Practitioner based in Castle Hill, Sydney. He holds a Bachelor of Health Science in Traditional Chinese Medicine from UTS and a Bachelor of Medical Sciences from Macquarie University, and is registered with AHPRA under the Chinese Medicine Board of Australia.
His approach draws on both Chinese medicine and biomedical understanding, with a particular interest in musculoskeletal conditions, stress-related presentations and internal health. He practises at Brandon Lau Acupuncture in Castle Hill and KO Healing Acupuncture in North Ryde.