
Low Back Pain and the Role of the Glutes: A Clinical Deep Dive
Low back pain is one of the most common presentations in clinic. It's also one of the most commonly misunderstood. Most people assume the pain originates from the back itself, and sometimes it does. But in a significant number of cases, the back is compensating for a problem that started somewhere else entirely.
Lower crossed syndrome: where the pattern begins
The most common functional pattern underlying chronic low back pain is lower crossed syndrome. Understanding it changes how the problem is approached.
Prolonged sitting shortens and tightens the psoas, a deep hip muscle that runs from the lumbar vertebrae through the pelvis and attaches to the femur. When the psoas is chronically tight it pulls the pelvis into anterior tilt, tipping it forward and down. This position inhibits the glutes, particularly gluteus medius, which is responsible for stabilising the pelvis during movement.
When the glutes stop doing their job, the surrounding muscles have to pick up the slack. The quadratus lumborum, the lumbar extensors and the piriformis become overloaded trying to maintain stability that the glutes should be providing. The lower back tightens, the hips lose mobility, and the pain that develops is felt in the back even though the back is the victim rather than the cause.
The broader hip flexor group, including the iliacus which works closely with the psoas, can also contribute to this pattern. In most cases addressing the psoas is sufficient to resolve the hip flexor component. Where there is specific tightness or soreness at the hip flexors directly, those muscles are worth assessing and treating separately.
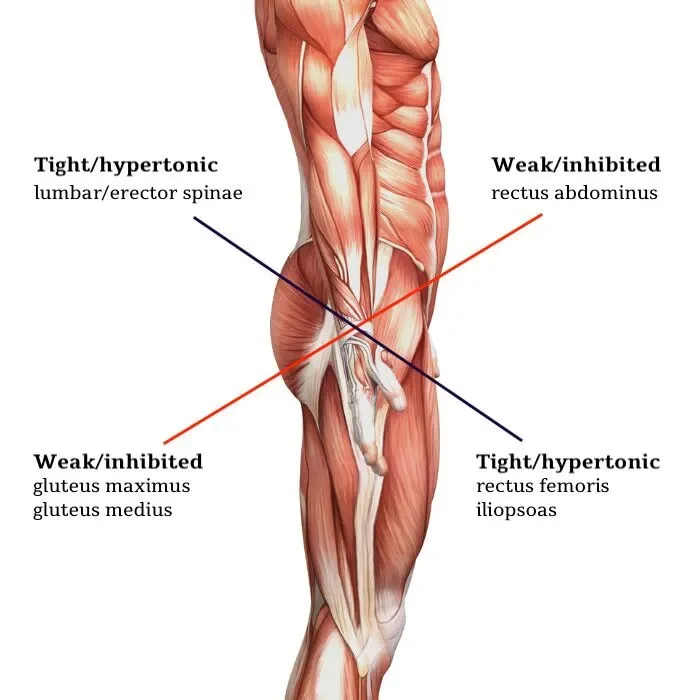
A visual representation of the lower crossed syndrome. Image Source: Yoganatomy
What this does to the disc
The muscle guarding that develops around a painful lower back compounds the problem. When the lumbar muscles are in constant spasm, they compress the spine and reduce the disc's ability to move freely. Intervertebral discs rely on movement and load cycling to draw in fluid and maintain their hydration. A spine held rigidly by overworked muscles can't cycle load effectively, which over time contributes to disc compression, reduced hydration and the conditions that precede disc bulging or herniation.
Releasing the muscle guarding is not just about reducing pain. It's about restoring the mechanical conditions that allow the disc to recover. This is why treating the musculature around the spine is clinically relevant even in cases where structural disc involvement is already present.
Recognising psoas involvement
The psoas is a deep muscle and can't be palpated directly in the way a superficial muscle can. Identifying its involvement relies on a combination of history and assessment findings.
The most consistent thing patients report is low back pain that worsens after prolonged sitting and eases once they get up and move around. This pattern makes sense anatomically. Sitting keeps the psoas in a shortened position. Getting up and walking allows it to lengthen slightly and temporarily reduces the compressive load on the spine.
Difficulty fully straightening the hip when standing is another indicator. A slight forward lean at the trunk, particularly noticeable when trying to stand fully upright, often reflects a psoas that is too tight to allow complete hip extension.
Some patients also find they cannot lie flat on their back comfortably. Placing a pillow or bolster under the knees relieves the pull at the lower back because it reduces the demand on the psoas to lengthen fully. If this is something a patient already does habitually, psoas involvement is worth investigating.
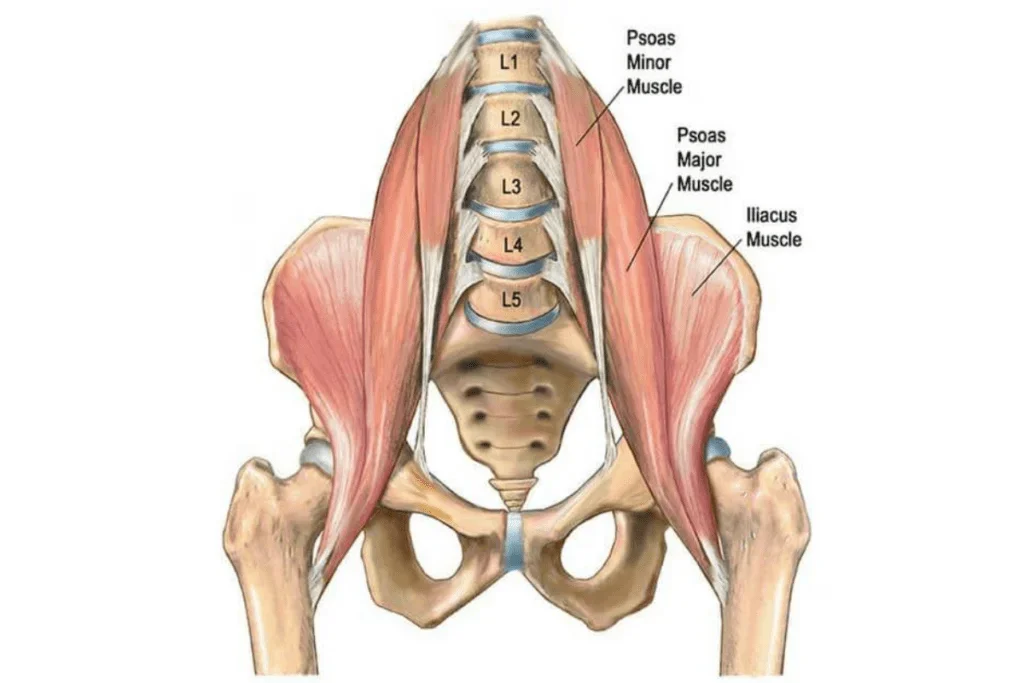
Image source: Movement Enhanced
Assessment in clinic
Before treatment begins, range of movement is assessed. Forward flexion, extension, lateral flexion and rotation give a picture of where restriction is greatest and which structures are most likely contributing. Hip internal and external rotation are also worth checking, since restriction here often points toward involvement of the deep hip rotators alongside the primary pattern.
From there, the muscle tone is assessed directly, checking for areas of tightness, trigger points and any referred pain on pressure. The combination of movement findings and palpation guides which muscles to prioritise in treatment.
What treatment involves
The approach here is primarily biomedical and sports acupuncture based. The focus is on the muscles directly rather than a traditional Chinese medicine channel approach, though the two are not mutually exclusive.
Motor point acupuncture targets the most electrically active point within a muscle, where the nerve meets the muscle tissue. Stimulating this point produces a stronger release response than needling a trigger point alone. Think of it like rebooting a frozen computer. The muscle receives a direct signal to reset its firing pattern, which helps restore normal tone and function.
For lower crossed syndrome, the muscles worth addressing through motor point acupuncture are:
Gluteus medius: The primary pelvic stabiliser. Releasing and reactivating this muscle is usually the most important part of the treatment.
Quadratus lumborum: The muscle most commonly overloaded when the glutes are inhibited. Often the direct source of the pain the patient feels.
Piriformis and deep hip rotators including obturator internus and gemelli: These become tight and overworked as part of the compensatory pattern and can contribute to sciatic nerve irritation if left unaddressed.
Lumbar extensors including longissimus: Worth including where there is significant lumbar tension and restricted extension.
Psoas: Addressed where there is clear clinical indication of its involvement. The psoas is a deep muscle located along the anterior aspect of the lumbar spine. Needling it requires precision but is well tolerated in most cases and can produce a significant release in patients where it is the primary driver of the pattern.
Electro stimulation is applied at the motor points. The approach varies depending on what the session calls for. Sometimes stimulation is applied early to wake the muscle up before allowing the needles to retain and relax. Other times, the needles retain for most of the session first and stimulation is applied toward the end. The sequencing is adapted to what makes the most clinical sense for that patient at that time rather than following a fixed order.
For patients new to acupuncture or motor point work specifically, the first session focuses on introducing the body to the technique before progressing to full stimulation.
What to expect when you visit
The first session starts with a conversation about the history of the pain, what makes it better or worse, and what daily activities are most affected. Movement is assessed before and after treatment so there is a clear before and after picture of what has shifted.
Most patients notice some change in how the back feels and how freely they can move by the end of the session. How much change and how lasting it is depends on how established the pattern is and how many contributing muscles are involved.
Lower crossed syndrome that has been present for years generally takes more consistent work to fully resolve than a recent onset case. The goal in the early sessions is to begin shifting the pattern and restoring some function. The goal over a course of treatment is to address the underlying imbalance thoroughly enough that the pattern stops reforming.
If low back pain is something you have been managing rather than resolving, it is worth coming in to assess what is actually contributing to it.

About Brandon Lau
Brandon is a registered Acupuncturist and Chinese Herbal Medicine Practitioner based in Castle Hill, Sydney. He holds a Bachelor of Health Science in Traditional Chinese Medicine from UTS and a Bachelor of Medical Sciences from Macquarie University, and is registered with AHPRA under the Chinese Medicine Board of Australia.
His approach draws on both Chinese medicine and biomedical understanding, with a particular interest in musculoskeletal conditions, stress-related presentations and internal health. He practises at Brandon Lau Acupuncture in Castle Hill and KO Healing Acupuncture in North Ryde.